
That Which Must Not Be Named
Saying out loud what we’re not supposed to talk about


For various reasons, I’m afraid to write this. One reason is that I don’t want to come off as “mean.” Another is that I don’t enjoy conflict, and I imagine that, once certain people read this, they will feel angry and want to lash out at me.
Ah, whatever.
This article is about autogynephilia.
Autogynephilia, for those who don’t know, is a sexual paraphilia. Autogynephilic (AGP) males are males who are sexually aroused by the thought of themselves as female. An abstract for a 2011 journal article by the psychologist and physician Anne Lawrence, a self-identified autogynephile, explained AGP well: “Autogynephilia exemplifies an unusual paraphilic category called 'erotic target identity inversions', in which men desire to impersonate or turn their bodies into facsimiles of the persons or things to which they are sexually attracted.” In this way, it is much like a sexual orientation. AGP males are attracted to, or even in love with, the women they imagine themselves to be.
The vast majority of adult trans-identified males (transwomen) are thought to be autogynephilic. A minority of adult trans-identified males are called “homosexual transsexuals” (HSTS). HSTS males are gay males who are naturally very effeminate and who feel more comfortable (and safer) identifying and attempting to live and pass as female. HSTS males have been gender-nonconforming their entire lives, since they first began expressing themselves as toddlers.
AGP males are typically the opposite. That is, they are and always have been very gender-conforming, often occupying roles in male-centric professions like law enforcement and the military.
HSTS males sometimes “pass” as women.
AGP males typically do not pass.1
OK. So, why am I writing about this?
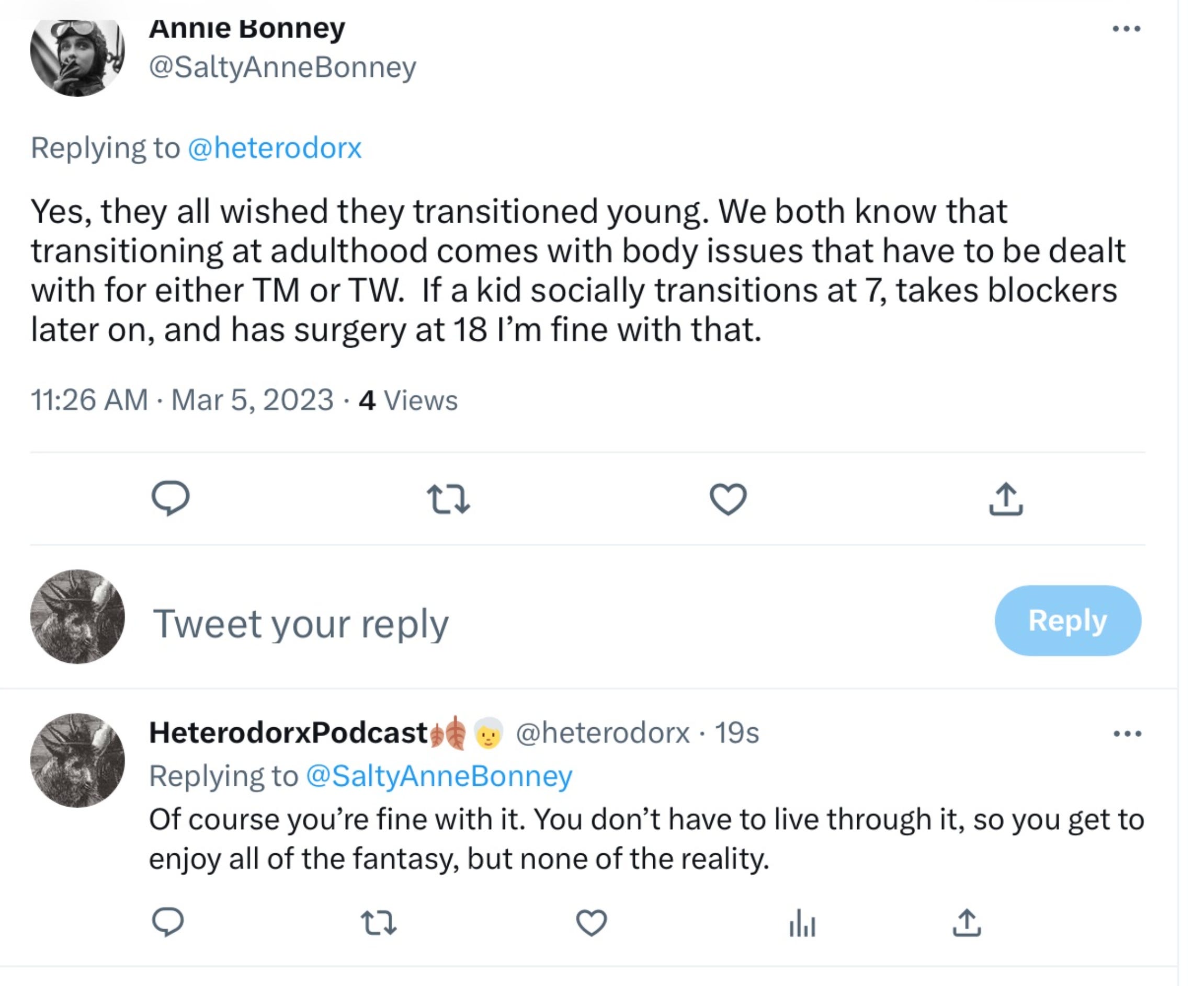
Because understanding the distinction between AGP and HSTS males is vital to protecting gender-nonconforming children, especially young boys, from the gender industry. The reason why it’s vital is best explained in a March 2023 thread by Cori Cohn (@heterodorx on X), an adult male who was “affirmed” as a teenager and underwent a sex-reassignment surgery at 19:
“I really wish I could make everyone understand that adult males who transition have persistent fantasies that they’d transitioned as children, and that the strain of activism aimed at boys is to experience this fantasy vicariously. I wish I could make everyone understand that there are some doctors and surgeons, even trans-identified ones within [World Professional Association for Transgender Health] WPATH leadership, who are complicit in materializing adult fantasies by sexually modifying boys. Transitioning boys especially is about the sexual gratification of adult men who project their wishes and regrets onto subjects who cannot consent to the actual process of medicalization. This is a tough truth to reckon with.”
To fully grasp what Cori is saying here, one must understand why the Dutch protocol (puberty blockers at 12, cross-sex hormones at 16, and surgery at 18 or later) was invented in the first place: to medically engineer effeminate young boys with gender identity disorder into adults who “pass” as women. Adult transwomen, the Dutch clinicians had observed, were often depressed and suicidal, which seemed to be related to their inability to pass. Thus, they thought, if they block a boy’s puberty, he won’t develop male secondary sex traits like broad shoulders and body hair, and if they give him estrogen, he’ll develop female secondary sex traits like breasts and softer skin. Once he’s castrated, they can take him off the blocker, since he’ll no longer have any gonads to produce testosterone!
The Dutch protocol leaves males sterile and often sexually nonfunctional; therefore, it’s a eugenics-ish way of making their possible future selves slightly less unhappy about their appearance.
The problem with all of this—besides the fact that it’s insane—is that the vast majority of the effeminate boys will desist (stop thinking they were supposed to be born as girls) once they commence through puberty, and the vast majority of those desisters will grow up to be gay men. The very few whose gender identity disorder (referred to today as “gender dysphoria”) persists might decide to medically transition as adults and attempt to live and pass as women. (If they do medicalize, they will belong to the HSTS cohort of transsexuals.)
There is no clinical test to determine which boys’ gender dysphoria will persist into adulthood and which boys’ will not persist. And since we cannot tell the future, there is no way to determine which boys will grow up to identify as gay—with their bodies and endocrine systems intact—and which boys will grow up to identify as transwomen. Therefore, it is totally unethical to subject young males to this protocol. It is, I believe, a violation of their human rights.

When I texted Cori to make sure he didn’t mind me quoting him in this article, he elaborated on his original Twitter/X thread. Cori wrote, “The key concept that I struggle to communicate—and I know this from having been the target of these men when I was young—is that their sexual desire is internally directed. They want boys to transition not out of desire for the boys, but to relieve their own unfulfillable fantasy of being that boy.”
So there you have it.
Am I writing this to inflict shame upon autogynephiles?
No.
Am I writing this because I think all autogynephiles are behind the push to medically transition (block puberty, administer synthetic hormones, and castrate) male children?
No.
But I do think that many of them are. And I find it despicable. An adult male whose life history and pathway to identifying as trans is entirely different from a gender-nonconforming boys’ experience should have absolutely no say in determining healthcare protocols for those boys. None. Especially when that adult male’s motivations are self-centered in this way.
And yes, Assistant Secretary for Health Rachel Levine, I’m looking at you. You married a woman and had children. You didn’t come out as a trans until you were in your fifties, as far as I understand it. You played football for your all-boys prep school, for God’s sake. You are and never were like the girly young boys that wrestle with deep internal shame about their same-sex attraction. That’s not to say you don’t know or have never known shame related to your sexuality. But it is not the same. You are not the same.
And no, of course I cannot be certain that Levine is AGP, though it is likely, since Levine fits the bill to a T. But what I can be certain of is Levine’s complicity in allowing this medical scandal to persist for as long as it has. Levine’s deplorable actions—for starters, his (sorry, can’t bring myself to use female pronouns for Levine) suppression of the findings of a Johns Hopkins systematic evidence review concerning the safety and efficacy of pediatric sex-trait modification and his pressuring of WPATH to remove age restrictions from their latest Standards of Care—alone should have led to the end of his career as assistant secretary for health and to the end of “gender-affirming care” for minors in the U.S.
Come to think of it, in recent years there have been at least a gazillion discoveries and events that should have ended these practices. But alas, the horror show goes on.
I didn’t really plan on writing about this topic today. But I saw something online last night that I can’t stop thinking about. It’s this screenshot that was posted by the writer Meghan Murphy of a Twitter/X exchange between political commentator Richard Hanania and Brianna Wu, a transwoman and the cofounder of a progressive political action committee:

If you don’t understand the exchange, Wu is implying that, if we want to create adult males who can pass as desirable women (like transwoman Hunter Schafer, apparently), then we should advocate for permanently blocking the natural development of girly little boys by giving them the same drugs that are used to chemically castrate adult male sex offenders.
This transsexual typology was developed by the sexologist Ray Blanchard in the 1980s. It only applies to males, though there is a similar, albeit less-established, typology for females. Forty years later, Blanchard’s typology still holds up, but obviously, with the huge uptick in trans identification in recent years (due to a whole host of debatable factors), there are now many other reasons why a person might identify as trans (social contagion, social cache, radical politics, etc.).
The distinction between AGPs and gender non-conforming ("girly") boys is also critical to women's and girls' safety and rights. The fact that transvestites/AGPs/fetishists have been included under the "trans" umbrella and treated as some kind of oppressed minority in need of expanded rights and cultural uplift has meant that politicians and media alike have gotten behind pushing these fetishistic straight men into women's and girls' private spaces, prisons, rape shelters, domestic violence shelters, and sports teams. The AGPs are having a field day with this, as entry into each of these spaces feeds into their fetish while eroding the rights of women and girls to privacy, dignity, and safety.
Thank you, Ben, for addressing the topic so calmly yet directly.
Question: Do you think we should drop the AGP label and just call it transvestic fetishism?
I feel like "autogynephilia" is a pseudomedical term that only draws us into arguments about whether AGP really exists and how many AGPs there are, distracting us from the actual point, which is this: Cross dressers -- ie, around 3% of adult men -- have been included under the trans umbrella and invited to flaunt and escalate their fetish while being lauded by the public as stunning and brave.